What is coronary heart disease (CHD)?
Coronary heart disease (CHD) refers to the narrowing of the coronary arteries in the heart due to the buildup of plaques in them. CHD can decrease the blood and thus oxygen and nutrients supply to the heart (ischemia), which can result in chest pain (angina pectoris) or heart attack.
Synonyms: coronary artery disease, ischemic heart disease
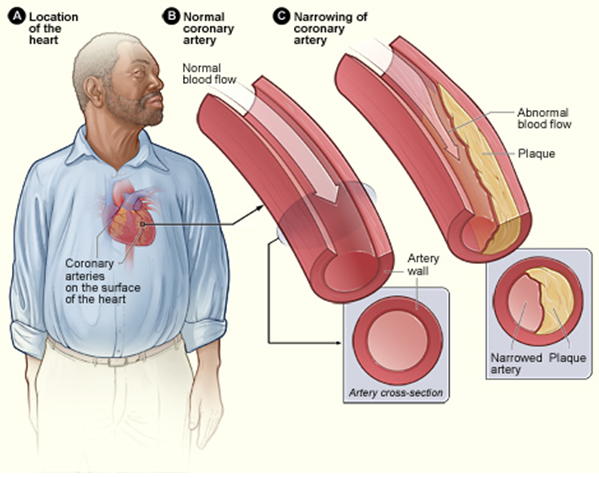
Picture 1. Coronary heart disease: normal and clogged coronary artery
(source: nhlbi.nih.gov, Public domain)
What are the coronary arteries?
Coronary arteries (from the Latin corona = crown or circle) are 2 arteries that originate from the aorta, run around the heart and supply the heart muscle with blood.
Causes and Risk Factors for CHD
The underlying condition in CHD is the hardening and narrowing (atherosclerosis) of the coronary arteries because of the buildup of plaques composed of cholesterol and calcium (atheroma).
Main controllable risk factors for CHD [1,2]:
- High LDL and low HDL cholesterol and high triglyceride levels
- Diabetes mellitus and prediabetes
- Overweight and obesity
- High blood pressure
- Cigarette smoking
- Lack of physical activity
- Psychological stress and depression
The particularly bad combination of risk factors for CHD, called metabolic syndrome, includes abdominal obesity, high blood pressure, high glucose and triglyceride and low HDL levels [2].
Main non-controllable risk factors for CHD [1,2]:
- Age >45 in men and >55 in women
- Genetic predisposition (family history of early CHD, race: African Americans, South Asians)
Other possible risk factors [2]:
- High levels of small dense LDL particles, homocysteine [77,78] and fibrinogen, and low testosterone levels
- Chronic inflammatory disease, such as systemic lupus erythematosus or rheumatoid arthritis [51]
- Too little or too much sleep
- “Screen time entertainment” (TV, computer, cinema)
- Vitamin D deficiency [84]
- End-stage kidney disease
- HIV/AIDS
There is conflicting evidence about high levels of C-reactive protein (CRP) [2,79,80,81] and lipoprotein(a) [82,83] as independent risk factors for CHD.
Symptoms of CHD
Coronary heart disease, especially in its early phase, can be present without any symptoms. Symptoms appear when the arterial plaques obstruct the delivery of blood and thus nutrients and oxygen to the heart. Initially, the pain appears only when the heart needs more oxygen, which is during exercise but later also during rest.
Individuals with CHD can experience recurrent chest pain called angina pectoris. A complete or prolonged blockage of the coronary arteries can cause the death of a part of the heart muscle, called myocardial infarct or heart attack.
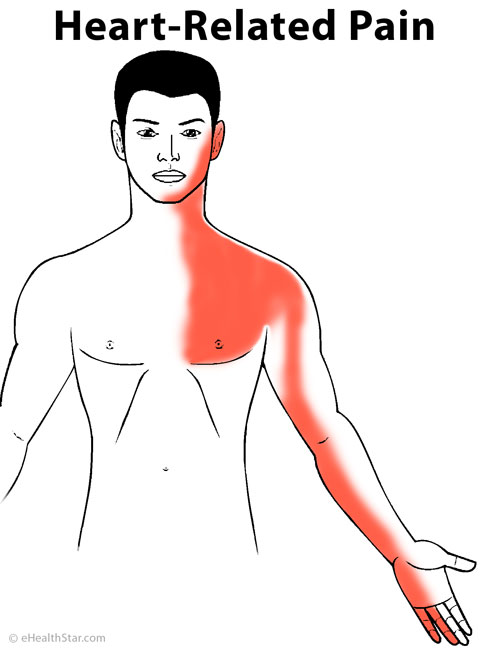
Picture 2. Pain distribution in coronary heart disease
(angina pectoris or heart attack)
Squeezing pain behind the sternum triggered by exercise, big meal, psychological stress or cold often radiates to the left shoulder blade, neck, jaw and down the inner side of the left arm all the way to the fingers. In women, pain often radiates into both or between the shoulder blades and both arms.
In angina pectoris, pain lasts less than 5 minutes and is quickly and completely relieved by rest or nitroglycerin.
In a heart attack, pain usually lasts more than 15 minutes, can be very severe and is not relieved by rest or nitroglycerin.
Other symptoms can include nausea, vomiting and fainting.
Diagnosis of CHD
A doctor can suspect coronary heart disease in a person with recurrent chest pain triggered by exercise.
The following investigations can reveal plaques in the coronary arteries [2,3]:
- Coronary angiogram or cardiac catheterization (an X-ray image of the coronary arteries after injecting a contrast substance into them)
- CT angiography
- Electron-beam computed tomography (EBCT)
- Carotid intima-media thickness (CIMT) test by using the ultrasound
- Stress testing (monitoring your heart rhythm and rate, blood pressure, chest pain, shortness of breath during exercise)
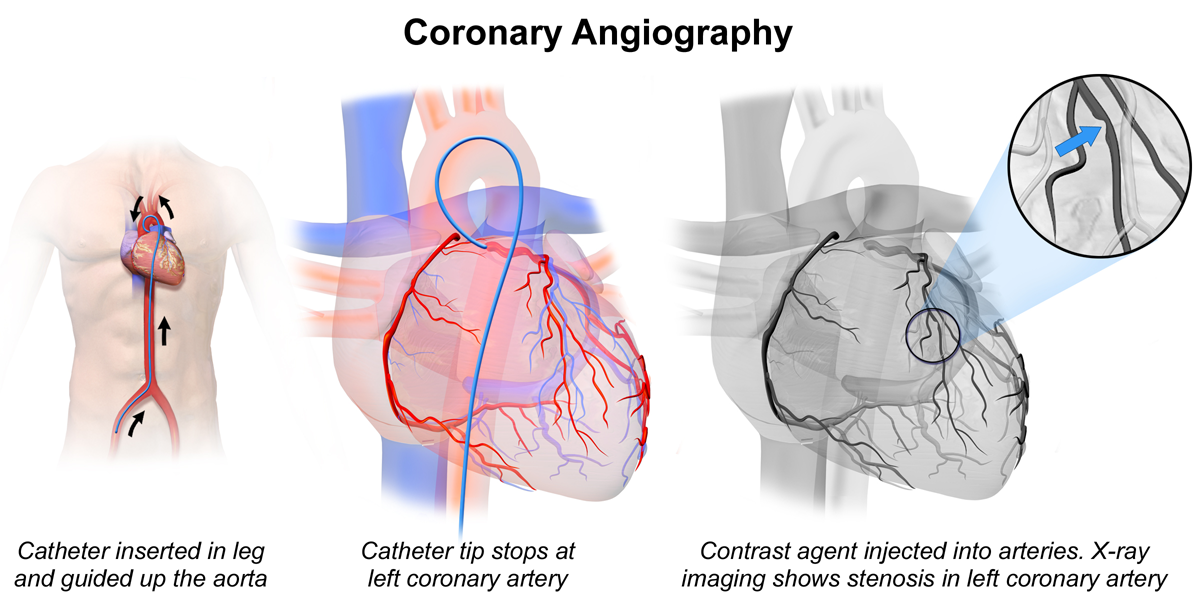
Picture 3. Coronary angiography
(source: Wikipedia, CC license)
{kind=link}
Differential Diagnosis
Conditions that can mimic coronary heart disease:
- Heart anxiety neurosis
- Trapped wind
- Costochondritis
- Peptic ulcer
- Pericarditis
- Pneumonia
- Pleurisy
- Pneumothorax
- Pulmonary embolism
Treatment of CHD
Currently, coronary heart disease cannot be cured, but it can be treated.
1. Drugs
Various combinations of drugs can be used in CHD:
- To reduce acute pain (angina pectoris): sublingual nitroglycerin (to apply under the tongue)
- To prevent pain by dilating coronary arteries and reducing oxygen demand by the heart: nitrates (isosorbide), beta-blockers (propranolol), calcium channel blockers (diltiazem, verapamil)
- To lower high LDL cholesterol: statins (lovastatin) [76]
- To raise low HDL cholesterol: niacin, fibrates (fenofibrate)
- To reduce blood clotting in the coronary arteries: aspirin or clopidogrel
- To lower high blood pressure:
- Angiotensin-converting enzyme (ACE) inhibitors, such as ramipril (They reduce the risk of complications of CHD, such as heart attack and death, even in individuals with normal blood pressure.) [75]
- Beta blockers can slow down the progression of the coronary heart disease [50].
- Ranolazine (anti-ischemic agent) can be used when other drugs are not effective [105].
- Reference: [75]
2. Supplements and Herbs
There is INSUFFICIENT EVIDENCE of the effectiveness of traditional Chinese herbal medicine in the treatment of heart-related chest pain (angina pectoris) [107].
3. Surgery
Balloon angioplasty is the widening of narrowed coronary arteries by the catheter that has an inflatable balloon and stent on end. A doctor inserts the catheter into the femoral artery in the groin and pushes it toward the heart. When the part of the catheter with the balloon and stent reaches the coronary arteries (which is checked by an X-ray), a doctor inflates the balloon and expands the stent. Then a doctor removes the catheter and the balloon, but the stent remains permanently in the artery and keeps it dilated [4]. This method is suitable when only one or few short parts of the arteries are narrowed.
Coronary artery bypass grafting (CABG) is a method of overcoming the narrowed parts of the coronary arteries by using a piece of an artery or vein (usually taken from a patient’s leg, arm or chest) and sewing it with one end in the aorta and the other end in the coronary artery after the narrowing, which enables the blood flow around the narrowing [4]. The bypass is usually done only in severely narrowed coronary arteries; more than one bypass can be done at the same time. Surgery usually results in immediate and complete pain relief [103]. Arterial grafts remain open longer than venous grafts [103]. 20-30% of the patients may need a second procedure within 10 years [104].
Prevention of CHD
What you can do to reduce the risk of coronary heart disease:
- Maintain a healthy body weight.
- Maintain normal glucose, cholesterol and triglyceride levels.
- Maintain normal blood pressure.
- Do not smoke and drink excessive amounts of alcohol.
- Be regularly physically active.
- Learn to cope with emotional stress.
1. Diet
In short:
- Maintain healthy body weight — this is probably the single most effective dietary approach to decrease the risk of CHD.
- There is no single nutrient, dietary supplement or food that would prevent CHD. Vegetarian and Mediterranean diet have been associated with decreased risk of CHD in some studies.
Evidence about the HARMFUL effects of nutrients/foods on CHD:
Trans fat. High consumption of trans fats from fast foods (French fries, cheeseburgers, chicken nuggets), commercially baked products (biscuits, crackers, doughnuts, pies), stick margarines, vegetable shortening, coffee creamers, other foods with added “partially hydrogenated oil” or Vanaspati ghee (clarified butter used in South Asia) have been associated with increased risk of CHD [5,6,7,8,9,23].
Saturated fat. According to some systematic reviews of studies, there is a strong association between high intake of saturated fat and CHD [11,12], but according to other reviews, there is insufficient evidence of such association [13,14,15,16,17,23]. High consumption of processed meat [85] was associated with increased risk of CHD, but consumption of unprocessed red meat (beef, pork, lamb) [85], dairy products [10] and specifically milk [87,88,89], cheese [87] or butter [87] and coconut oil [90,91] was not. Some researchers have suggested that preservatives in processed meat, such as sodium, nitrites, nitrates and nitrosamines, may increase the risk of CHD [85].
Sodium. There is CONFLICTING EVIDENCE about high sodium intake as a risk factor for CHD [18,19,20,21,97]. According to one review, high sodium intake is associated with increased risk of CHD only in individuals with hypertension [22].
There is NO CONVINCING EVIDENCE that high cholesterol (eggs, shrimps, organ meats) [47,48,49] total fat [52,53,54] added sugars (soft drinks, sweets) [102] or, specifically, fructose [43] intake would increase the risk of CHD. NOTE: High sugar and fat intake often lead to obesity, which is a risk factor for CHD.
Evidence of the PREVENTATIVE effects of nutrients, supplements or herbs on CHD:
Fish. There is SOME EVIDENCE that consumption of fatty fish high in omega-3 polyunsaturated fatty acids EPA and DHA (mackerel, salmon, sardines, halibut, trout), at least once to twice weekly [35], but less likely fish oil supplements [35,37,41,109] decreases the risk of CHD. NOTE: Fish oil may decrease the risk of CHD only in people with known risk factors (obesity, high LDL cholesterol and triglycerides) [37]. In people who regularly consume fish, fish oil probably does not have any additional heart-protecting effect [37].
There is SOME EVIDENCE that replacing some saturated fat with polyunsaturated fats in the diet can reduce the risk of CHD [38,39,40].
Whole grains. There is SOME EVIDENCE that regular intake of insoluble dietary fiber from whole-grain cereals and vegetables [55], beta-glucan from whole barley and oats [56,108] or psyllium husk (at least 7 g/day) [57] is associated with the lower risk of CHD.
Vegetarian and Mediterranean diet. According to 3 reviews of observational studies, vegetarians had 25-34% lower mortality from ischemic heart disease than regular meat eaters [63,64,65]. Mediterranean diet (regular consumption of whole grains, fish, poultry, vegetables, beans, potatoes, fruits, olive oil, nuts, seeds and wine) was also associated with lower risk of CHD [66,67,68,69,70].
Moderate alcohol drinking (up to 2 drinks per day for men and 1 drink per day for women) was associated with decreased risk of CHD when compared with excessive drinking or not drinking at all [28,29,30]. There is not enough evidence to claim that red wine (high in polyphenols) is more effective in the prevention of CHD than other alcoholic beverages [27].
There is INSUFFICIENT EVIDENCE of the preventative effect of high intake or supplementation of any nutrient or herb, such as coenzyme Q10 [31], antioxidants or vitamins A, C, D, E [45], B6, B12 or folate [44], choline [46], flavanols in green or black tea [32], soy isoflavones [36], resveratrol [33], garlic [96], phytosterols [97,98], alpha-linolenic acid from flaxseed oil [34], potassium [60], calcium [59], magnesium [58], chocolate or cocoa (high in polyphenols [100,101], Tong-xin-luo capsules [106] or monounsaturated fatty acids from olive oil or nuts [40,42] on CHD.
There is INSUFFICIENT EVIDENCE of the preventative effect of a low-carb [71,72] or low glycemic index diet [62] on CHD.
2. Exercise
There is SOME EVIDENCE that regular physical exercise (at least 30 min/day) may decrease the risk of CHD [92], possibly because it helps to maintain healthy body weight, increase HDL and decreased LDL cholesterol and triglyceride levels [93,95] and decreases the risk of diabetes 2 (insulin resistance) [94].
There is INSUFFICIENT EVIDENCE of the preventative effect of yoga on CHD [61].
3. Drugs
Aspirin, taken regularly, can modestly decrease the risk of CHD [73,74].
Caffeine does not seem to decrease or increase the risk of CHD [24,25,26].
- References
- What Are Coronary Heart Disease Risk Factors? National Heart, Lung and Blood Institute
- Bodi FB, Risk factors for coronary heart disease Emedicine
- How is coronary heart disease diagnosed? National Heart, Lung and Blood Institute
- Michaels AD et al, 2002, Angioplasty Versus Bypass Surgery for Coronary Artery Disease Circulation
- Mozaffarian D et al, 2006, Trans Fatty Acids and Cardiovascular Disease The New England Journal of Medicine
- Teegala SM et al, 2009, Consumption and health effects of trans fatty acids: a review PubMed
- Mente A et al, 2009, A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease PubMed
- Ascherio A et al, 1999, Trans Fatty Acids and Coronary Heart Disease The New England Journal of Medicine
- 2007, Opinion of the Scientific Panel on Dietetic products, nutrition and allergies [NDA] related to the presence of trans fatty acids in foods and the effect on human health of the consumption of trans fatty acids European Food Safety Authority
- Mullie P et al, 2016, Daily milk consumption and all-cause mortality, coronary heart disease and stroke: a systematic review and meta-analysis of observational cohort studies PubMed Central
- 2002, Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Circulation
- Dietary fats: Total Fat and Fatty Acids US Department of Agriculture
- Siri-Tarino PW et al, 2010, Saturated Fatty Acids and Risk of Coronary Heart Disease: Modulation by Replacement Nutrients PubMed Central
- Hooper L et al, 2001, Dietary fat intake and prevention of cardiovascular disease: systematic review The BMJ
- Mente A et al, 2009, A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease PubMed
- Chowdhury R et al, 2014, Association of Dietary, Circulating, and Supplement Fatty Acids With Coronary Risk: A Systematic Review and Meta-analysis Annals of Internal Medicine
- Hoenselaar R, 2011, Saturated fat and cardiovascular disease: The discrepancy between the scientific literature and dietary advice Nutrition
- Sodium Linus Pauling Institute
- Aburto NJ et al, 2013, Effect of lower sodium intake on health: systematic review and meta-analyses PubMed
- Stamler J, INTERSALT study, 1984-1997 University of Minnesota
- 2012, Effects of reduced sodium intake on cardiovascular disease, coronary heart disease and stroke World Health Organization
- Joosten MM et al, 2014, Sodium excretion and risk of developing coronary heart disease PubMed
- de Souza RJ et al, 2015, Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies The BMJ
- 2012, Regular, moderate, coffee drinking may reduce heart failure risk Heart.org
- Ding M et al, 2014, Long-Term Coffee Consumption and Risk of Cardiovascular Disease: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies PubMed
- Greenberg JA et al, 2007, Caffeinated beverage intake and the risk of heart disease mortality in the elderly: a prospective analysis The American Journal of Clinical Nutrition
- Brien SE et al, 2011, Effect of alcohol consumption on biological markers associated with risk of coronary heart disease: systematic review and meta-analysis of interventional studies PubMed Central
- Alcoholic beverages Linus Pauling Institute
- Hein HO et al, 1997, Alcohol consumption, S-LDL-cholesterol and risk of ischemic heart disease. 6-year follow-up in The Copenhagen Male Study PubMed
- Mukamal KJ et al, 2003, Alcohol consumption and carotid atherosclerosis in older adults: the Cardiovascular Health Study PubMed
- Coenzyme Q10, evidence Mayo Clinic
- Hartley R et al, 2013, Green and black tea to prevent cardiovascular disease Cochrane
- Sahebkar A et al, 2015, Lack of efficacy of resveratrol on C-reactive protein and selected cardiovascular risk factors–Results from a systematic review and meta-analysis of randomized controlled trials PubMed
- Flaxseed oil WebMD
- Omega-3 supplements: in depth National Center for Complementary and Integrative Health
- Soy WebMD
- Kris-Etherton PM et al, 2002, Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease Circulation
- Hooper L et al, 2015, Effect of cutting down on the saturated fat we eat on our risk of heart disease Cochrane
- Mozaffarian D et al, 2010, Effects on coronary heart disease of increasing polyunsaturated fat in place of saturated fat: a systematic review and meta-analysis of randomized controlled trials PubMed
- Siri-Tarino PW et al, 2010, Saturated Fatty Acids and Risk of Coronary Heart Disease: Modulation by Replacement Nutrients PubMed Central
- Rizos EC et al, 2012, Association between omega-3 fatty acid supplementation and risk of major cardiovascular disease events: a systematic review and meta-analysis PubMed
- Schwingshackl L et al, 2012, Monounsaturated Fatty Acids and Risk of Cardiovascular Disease: Synopsis of the Evidence Available from Systematic Reviews and Meta-Analyses PubMed Central
- Tappy L et al, 2010, Metabolic Effects of Fructose and the Worldwide Increase in Obesity Physiological Reviews
- Myung S-K et al, 2013, Efficacy of vitamin and antioxidant supplements in prevention of cardiovascular disease: systematic review and meta-analysis of randomised controlled trials The BMJ
- Vitamin E evidence Mayo Clinic
- Choline WebMD
- Kratz M, 2005, Dietary cholesterol, atherosclerosis and coronary heart disease PubMed
- Shin JY et al, 2013, Egg consumption in relation to risk of cardiovascular disease and diabetes: a systematic review and meta-analysis PubMed Central
- Rong Y et al, 2013, Egg consumption and risk of coronary heart disease and stroke: dose-response meta-analysis of prospective cohort studies The BMJ
- Siphai I et al, 2007, Beta-blockers and progression of coronary atherosclerosis: pooled analysis of 4 intravascular ultrasonography trials PubMed
- Rheumatoid arthritis, clinical presentation Emedicine
- Schwab U et al, 2014, Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: a systematic review PubMed Central
- Hooper L et al, 2012, Effect of reducing total fat intake on body weight: systematic review and meta-analysis of randomised controlled trials and cohort studies PubMed Central
- Mente A et al, 2009, A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease PubMed
- Threapleton, DE et al, 2013, Dietary fibre intake and risk of cardiovascular disease: systematic review and meta-analysis The BMJ
- §101.81 Health claims: Soluble fiber from certain foods and risk of coronary heart disease (CHD) Electronic Code of Federal Regulations
- Bernstein AM et al, 2013, Major Cereal Grain Fibers and Psyllium in Relation to Cardiovascular Health PubMed Central
- Magnesium Linus Pauling Institute
- Calcium intake and risk of cardiovascular disease PubMed
- 2012, Potassium intake for adults and children World Health Organization
- Kwong JSW et al, 2015, Yoga for secondary prevention of coronary heart disease Cochrane
- Kelly SAM et al, 2004, Low glycaemic index diets for coronary heart disease Cochrane
- Key TJ et al, 1999, Mortality in vegetarians and nonvegetarians: detailed findings from a collaborative analysis of 5 prospective studies The American Journal of Clinical Nutrition
- Dinu M et al, 2016, Vegetarian, vegan diets and multiple health outcomes: a systematic review with meta-analysis of observational studies PubMed
- Huang T et al, 2012, Cardiovascular disease mortality and cancer incidence in vegetarians: a meta-analysis and systematic review PubMed
- Buckland G et al, 2009, Adherence to the Mediterranean diet and risk of coronary heart disease in the Spanish EPIC Cohort Study PubMed
- Martínez-González MA et al, 2011, Mediterranean diet and the incidence of cardiovascular disease: a Spanish cohort PubMed
- Mente A et al, 2009, A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease PubMed
- Fidanza F et al, 2004, Mediterranean Adequacy Index: correlation with 25-year mortality from coronary heart disease in the Seven Countries Study PubMed
- Panagiotakos DB et al, 2004, Can a Mediterranean diet moderate the development and clinical progression of coronary heart disease? A systematic review. PubMed
- Naude CE et al, 2014, Low carbohydrate versus isoenergetic balanced diets for reducing weight and cardiovascular risk: a systematic review and meta-analysis PubMed
- Santos FL et al, 2012, Systematic review and meta-analysis of clinical trials of the effects of low carbohydrate diets on cardiovascular risk factors PubMed
- Sutcliffe P et al, 2013, Aspirin for prophylactic use in the primary prevention of cardiovascular disease and cancer: a systematic review and overview of reviews PubMed
- Brottons C et al, 2015 et al, A Systematic Review of Aspirin in Primary Prevention: Is It Time for a New Approach? PubMed Central
- Alaeddini J, Angina pectoris treatment & management Emedicine
- Yan YL et al, 2013, Efficacy and safety evaluation of intensive statin therapy in older patients with coronary heart disease: a systematic review and meta-analysis PubMed
- Ganguly P et al, 2015, Role of homocysteine in the development of cardiovascular disease PubMed Central
- Harish RB et al, 2007, Risk prediction—Homocysteine in Coronary Heart Disease PubMed Central
- C Reactive Protein Coronary Heart Disease Genetics Collaboration (CCGC), 2011, Association between C reactive protein and coronary heart disease: mendelian randomisation analysis based on individual participant data PubMed Central
- Shrivastava AK et al, 2015, C-reactive protein, inflammation and coronary heart disease ScienceDirect
- Strang F et al, 2014, C-Reactive Protein and Coronary Heart Disease: All Said—Is Not It? Hindawi
- Jacobson TA, 2013, Lipoprotein(a), cardiovascular disease, and contemporary management PubMed
- Malaguarnera M et al, 2013, Lipoprotein(a) in Cardiovascular Diseases Hindawi
- Siadat ZD et al, 2012, Association of vitamin D deficiency and coronary artery disease with cardiovascular risk factors PubMed Central
- Micha R et al, 2010, Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: a systematic review and meta-analysis PubMed Central
- Rice BH, 2014, Dairy and Cardiovascular Disease: A Review of Recent Observational Research PubMed Central
- Huth PJ et al, 2012, Influence of Dairy Product and Milk Fat Consumption on Cardiovascular Disease Risk: A Review of the Evidence Advances in Nutrition
- Mente A et al, 2009, A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease JAMA Internal Medicine
- Elwood PC et al, 2010, The Consumption of Milk and Dairy Foods and the Incidence of Vascular Disease and Diabetes: An Overview of the Evidence PubMed Central
- Lipoeto NI et al, 2004, Dietary intake and the risk of coronary heart disease among the coconut-consuming Minangkabau in West Sumatra, Indonesia PubMed
- Palazhy S et al, 2012, Composition of plasma and atheromatous plaque among coronary artery disease subjects consuming coconut oil or sunflower oil as the cooking medium PubMed
- Batty GD et al, 2002, Physical activity and coronary heart disease in older adults. A systematic review of epidemiological studies PubMed
- Mann S et al, 2014, Differential Effects of Aerobic Exercise, Resistance Training and Combined Exercise Modalities on Cholesterol and the Lipid Profile: Review, Synthesis and Recommendations PubMed Central
- Colberg SR et al, 2010, Exercise and Type 2 Diabetes, The American College of Sports Medicine and the American Diabetes Association: joint position statement PubMed Central
- Escalante Y et al, 2012, Improvement of the lipid profile with exercise in obese children: a systematic review PubMed
- Qidwai W et al, 2013, Role of Garlic Usage in Cardiovascular Disease Prevention: An Evidence-Based Approach PubMed
- Genser B et al, 2012, Plant sterols and cardiovascular disease: a systematic review and meta-analysis PubMed
- Gupta AK et al, 2011, Role of phytosterols in lipid-lowering: current perspectives QJM
- 2013, Sodium Intake in Populations: Assessment of Evidence National Academics
- Ding EL, Hutfless SM, Ding X, Girota S, 2006, Chocolate and Prevention of Cardiovascular Disease: A Systematic Review PubMed
- Khawaja O et al, 2011, Chocolate and coronary heart disease: a systematic review PubMed
- Malik VS et al, 2010, Sugar Sweetened Beverages, Obesity, Type 2 Diabetes and Cardiovascular Disease risk PubMed Central
- Aroesti JM, 2016, Patient information: Coronary artery bypass graft surgery (Beyond the Basics) UpToDate
- Coronary artery bypass Texas Heart Institute
- Alaeddini J, Angina pectoris medication Emedicine
- Mao C et al, 2015, Tong-xin-luo capsule for patients with coronary heart disease after percutaneous coronary intervention Cochrane
- Zhuo Q et al, 2010, This review did not find strong evidence to demonstrate the effect of traditional Chinese herbal products in the treatment of stable angina Cochrane
- Kelly SAM et al, 2007, Wholegrain cereals for coronary heart disease Cochrane
- Mohebi-Nejad A et al, 2014, Omega-3 Supplements and Cardiovascular Diseases PubMed Central